

“The biggest story is not just the Ebola outbreak. It’s really what it is revealing to us about misinformation, how dangerous that can be. It’s even sometimes worse than the disease.” Those words from journalist and Immigrant Magazine publisher Pamela Asobo-Anchang captured one of the central messages emerging from a recent national briefing on the growing Ebola outbreak in Central Africa. While medical experts are working to contain the virus, community leaders say misinformation, fear, and stigma could become equally dangerous obstacles.
A Serious but Contained Health Crisis
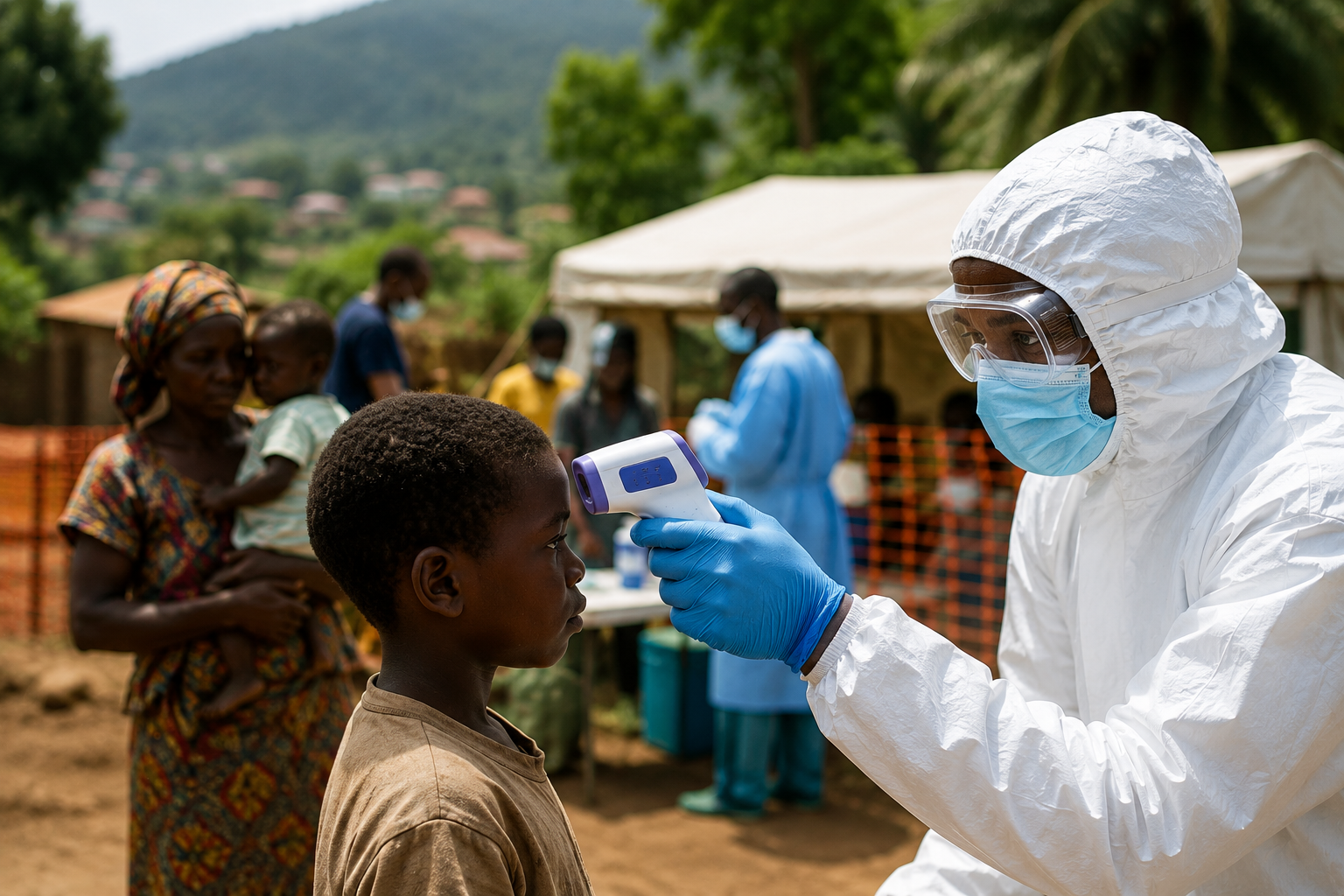
The current Ebola outbreak in the Democratic Republic of the Congo and neighboring Uganda is being driven by the rare Bundibugyo strain of the virus. According to health experts, this outbreak has already spread across several provinces and crossed international borders, making it one of the most significant Ebola emergencies in recent years.
Dr. William Schaffner, professor of preventive medicine and infectious diseases at Vanderbilt University School of Medicine, explained that Ebola belongs to a family of viral hemorrhagic fevers that naturally circulate in fruit bats. Human infection can occur through exposure to infected wildlife before the virus spreads from person to person through direct contact with the bodily fluids of someone who is seriously ill or has died from the disease.
Early symptoms often resemble many common illnesses, including fever, headache, muscle pain, weakness, and loss of appetite. As the disease progresses, patients may experience vomiting, diarrhea, dehydration, organ failure, and, in some cases, severe bleeding. Dr. Schaffner emphasized that patients are not contagious during the incubation period, but become highly infectious once symptoms progress and body fluids contain large amounts of the virus.
There is currently no approved vaccine specifically for the Bundibugyo strain, although researchers are working to develop one. For now, health officials rely on rapid diagnosis, patient isolation, contact tracing, and community education to stop transmission.
Separating Facts from Fear
Despite alarming headlines, Dr. Schaffner reassured Americans that the current risk to the United States remains very low.
“I will continue to emphasize that the risk to the United States population and to the developed world is very low,” he said. “This is not a respiratory virus. It is not transmitted the way influenza and COVID-19 viruses were.”
That distinction is important. Ebola does not spread through casual contact, the air, or simply being near someone. Transmission requires direct exposure to infected bodily fluids. Understanding these facts can help reduce unnecessary fear while encouraging appropriate vigilance.
Conflict Complicates the Response
Containing Ebola is not simply a medical challenge.
Dr. Rachel Sweet, a conflict researcher specializing in Central Africa, explained that ongoing violence and political instability make public health efforts far more difficult. Communities living under years of armed conflict often distrust government authorities and outside organizations, making it harder for health workers to gain cooperation during outbreaks.
“The main mechanism that drives mistrust,” she explained, is rooted in people’s lived experiences rather than ignorance. Understanding those realities is essential to building trust and encouraging communities to participate in lifesaving public health measures.
She also highlighted the remarkable dedication of local doctors, nurses, pastors, and community leaders who continue working despite limited resources and personal danger.
“I would close by emphasizing the widespread mobilization by on-the-ground community actors,” Sweet said, noting that many healthcare workers continue serving because they deeply care about their communities.
The Diaspora’s Responsibility
Perhaps the most compelling perspective came from Pamela Asobo-Anchang, who interviewed members of African immigrant communities across the United States.
She discovered dramatically different reactions. Some communities questioned whether the outbreak was as serious as reported, while others, particularly people with ties to the Democratic Republic of the Congo, expressed deep anxiety about family members, fragile healthcare systems, and the loss of international assistance.
Many feared another consequence beyond the disease itself.
“Stigma is the big, big problem,” Asobo-Anchang observed, recalling stories of Africans who experienced discrimination during previous Ebola outbreaks. Some immigrants worry that simply identifying themselves with affected countries could expose them to prejudice or even jeopardize employment opportunities.
She also found that many diaspora members are helping individually by sending money to relatives for food, clean drinking water, and medical needs. However, she believes those efforts need greater coordination.
“The diaspora has always supported the continent financially, resource-wise, and advocacy-wise,” she said. “Maybe our problem is that we’re doing it individually, but we need to do it collectively.”
A Christian Response
For Christians and immigrant communities, this crisis offers an opportunity to demonstrate compassion guided by wisdom.
Diaspora communities can play a vital role by sharing accurate health information, resisting rumors and superstition, supporting trusted humanitarian and medical organizations, checking in on family members regularly, encouraging local churches to pray and raise awareness, and advocating for long-term investments in healthcare infrastructure rather than responding only during emergencies.
The Ebola outbreak reminds us that diseases do not respect borders, but neither do compassion, generosity, or truth. Fighting misinformation is just as important as fighting the virus itself.
As Asobo-Anchang concluded, “The African diaspora is really willing and has a compassion to help. But we just need support in coordination and, you know, to make it count.”